
Colpocleisis
El prolapso de la vagina o el útero es una condición común. Hasta 11% de las mujeres requieren cirugía durante su vida para esta condición. El prolapso frecuentemente resulta a través de daño a las estructuras de soporte del útero y la vagina.
Los síntomas asociados con el prolapso incluyen una sensación de pesadez en la vagina o una protuberancia externa que se extiende fuera de la vagina. Puede causar una sensación de peso en la vagina o dolor de espalda baja y dificultad al pasar la orina o las heces.
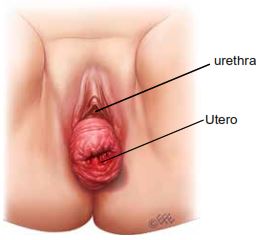
Aspecto antes del colpocleisis
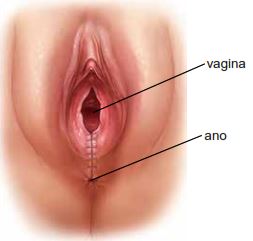
Aspecto después del colpocleisis
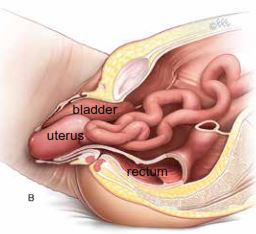
Aspecto antes del colpocleisis
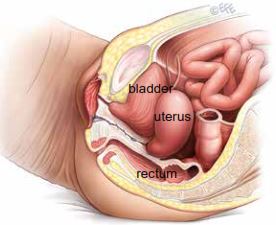
Aspecto después del colpocleisis
In this Health Topic
El colpocleisis es una operación que trata los síntomas de prolapso juntando las paredes delantera y trasera de la vagina. Esto evita que las paredes vaginales se salgan afuera de la vagina. Colpocleisis sólo es adecuado para las mujeres que no son activas sexualmente (y no tienen la intención de ser activas sexualmente en el futuro), ya que al cerrar el canal vaginal no se permite relaciones sexuales por la vagina.
El colpocleisis puede llevarse a cabo con mayor rapidez comparado con otros procedimientos de reconstrucción vaginal para el prolapso. Por consiguiente, es especialmente adecuado para las mujeres con problemas médicos que serían menos adecuadas para operaciones más largas y más complejas. Es asociado con altas tasas de éxito (90-95 %) y también es una opción para las mujeres que no son activas sexualmente que tienen prolapso recurrente después de cirugías previas . Puede ser realizado en mujeres con o sin útero.
Se le preguntará sobre su estado de salud general y los medicamentos que está tomando. Se coordinará las pruebas necesarias (por ejemplo, análisis de sangre, electrocardiograma, radiografía del pecho) . También recibirá información sobre su estadía en el hospital, la operación y el cuidado pre- y posoperatorio.
Cuando se despierte de la anestesia tendrá un suero para administrarle líquidos intravenosos y tendrá un catéter en la vejiga. El catéter generalmente se quita en 24 a 48 horas después de la operación. Usted será capaz de orinar normalmente después de un colpocleisis como la apertura a la vejiga está por encima de la apertura vaginal y por lo tanto no es afectada por el procedimiento.
Es normal tener una secreción de color blanca o amarillo cremoso de 4 a 6 semanas después de la cirugía. Esto es debido a la presencia de puntos en la vagina. Al absorberse los puntos, la secreción se reducirá gradualmente. Si la secreción tiene un mal olor, póngase en contacto con su médico. Usted puede tener un poco de flujo manchado con sangre inmediatamente después de la cirugía y la semana después de la cirugía . Esta sangre suele ser mínima, de color marrón y resulta del cuerpo rompiendo la sangre atrapada debajo de la piel.
Con cualquier operación siempre hay un riesgo de complicaciones. Las siguientes complicaciones generales pueden ocurrir después de cualquier cirugía:
- Problemas anestésicos. Con los anestésicos modernos y equipo de monitoreo, las complicaciones debidas a la anestesia son muy raras. La cirugía se puede realizar con anestesia espinal o general. Su anestesiólogo le explicará cuál es más adecuada para usted.
- El sangrado. La hemorragia grave que requiera transfusión de sangre es raro después de la cirugía vaginal.
- Infección quirúrgica. Aunque a menudo los antibióticos se dan justo antes de la cirugía y la cirugía se mantiene estéril, hay una pequeña probabilidad de contraer una infección en la vagina o la pelvis . Los síntomas incluyen flujo vaginal con olor desagradable, fiebre y dolor pélvico o malestar abdominal. Si tiene fiebre o secreciones con mal olor, póngase en contacto con su médico.
- Infecciones de la vejiga (cistitis) ocurren en aproximadamente 6 % de las mujeres después de la cirugía y son más comunes en casos que utilicen un catéter. Los síntomas incluyen ardor al orinar, frecuencia urinaria y sangre en la orina en ocasiones. La cistitis es usualmente fácilmente tratada con un ciclo de antibióticos.
- Los coágulos en los vasos sanguíneos de las piernas/ pulmones son más frecuentes en los pacientes sometidos a cirugía pélvica. Se le dará medias de compresión para reducir estos riesgo, y posiblemente una serie de inyecciones.
Las complicaciones relacionadas específicamente con colpocleisis
- Un hematoma se refiere a una acumulación de sangre que se forma debajo de los tejidos vaginales debido a la hemorragia de las superficies que hansido cosidas juntas. Esto puede causar dolor y un
sangrado más pesado y prolongado de lo esperado. Un hematoma también puede infectarse. La mayoría de los hematomas se resolverán por sí mismos. En raras ocasiones puede que tenga que tener otra operación para que los puntos se abran para permitir que el hematoma drene. - El estreñimiento es un problema común y el médico puede recetar suavizantes de heces o laxantes. Usted debe tratar de mantener una dieta alta en fibra y beber mucho líquido para ayudar también.
- Daño a la vejiga o al intestino son complicaciones poco frecuentes de la cirugía del prolapso vaginal.
Si usted tiene una operación de colpocleisis y el útero no se ha extraído, puede ser difícil para su médico investigar de donde viene un sangrado anormal de la vagina, una vez que la operación haya sanado. Si usted tiene sangrado anormal después de la operación y todavía tiene un útero asegúrese de que su proveedor médico sepa el tipo de operación que ha tenido, ya que una prueba de Papanicolaou del cuello del útero o una biopsia del útero probablemente no será posible. Evaluación sonográfica de las paredes del útero sigue siendo posible, pero no es tan precisa al diagnosticar el cáncer como lo es una biopsia. Si usted ha tenido un resultado anormal de la prueba de Papanicolaou del cuello uterino usted debe de hablar de esto con su cirujano antes de la operación.
Usted debe ser capaz de conducir y hacer actividades ligeras tales como paseos cortos algunas semanas después de la cirugía. Recuerde que debe aumentar su nivel de actividad gradualmente. Le aconsejamos que evite levantar objetos pesados y el deporte por al menos 6 semanas para permitir que las heridas sanen. Si usted trabaja, generalmente es aconsejable planear tomar de 4 a 6 semanas de descanso.
Su médico puede guiarla ya que esto dependerá de su tipo de trabajo y de la cirugía que ha tenido.
Para obtener más información, consulte el folleto de Prolapso de Organos Pélvicos o visite nuestro sitio de web en www.iuga.org y haga clic en la sección de información del paciente.