
Pelvic Organ Prolapse
In this Health Topic
This condition refers to the bulging or herniation of one or more pelvic organs into or out of the vagina. The pelvic organs consist of the uterus, vagina, bowel, and bladder. Pelvic organ prolapse occurs when the muscles, ligaments and fascia (a network of supporting tissue) that hold these organs in their correct positions become weakened.
Symptoms include:
- A heavy dragging feeling in the vagina or lower back
- Feeling of a lump in the vagina or outside the vagina
- Urinary symptoms such as slow urinary stream, a feeling of incomplete bladder emptying, urinary frequency or urgent desire to pass urine, and urinary stress incontinence
- Bowel symptoms, such as difficulty moving the bowel or a feeling of not emptying properly, or needing to press on the vaginal wall to empty the bowel
- Discomfort during sexual intercourse
The main cause is damage to the nerves, ligaments and muscles which support the pelvic organs and may result from the following:
- Pregnancy and childbirth are considered to be major factors leading to weakening of the vagina and its supports. Prolapse affects about one in three women who have had one or more children. A prolapse may occur during or shortly after a pregnancy or may take many years to develop. However, it is important to emphasize that only 1 out of 9 women (11%) will ever need surgery for prolapse in their lifetime.
- Aging and menopause may cause further weakening of the pelvic floor structures.
- Conditions that cause excessive pressure on the pelvic floor like obesity, chronic cough, chronic constipation, heavy lifting and straining.
- Some women may have an inherited risk for prolapse, while some diseases affect the strength of connective tissue, e.g. Marfan syndrome and Ehlers-Danlos syndrome.
A prolapse may arise in the front wall of the vagina (anterior compartment), back wall of the vagina (posterior compartment), the uterus and/or top of the vagina (apical compartment). Many women have a prolapse in more than one compartment at the same time.
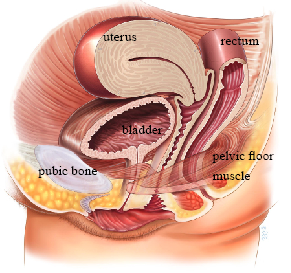
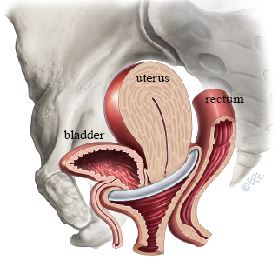
Normal Anatomy – No Prolapse
Prolapse of the Anterior Compartment
This is the most common type of prolapse and involves the bladder and/or urethra bulging into the vagina. Your doctor may refer to it as cystocele or cysto-urethrocele.
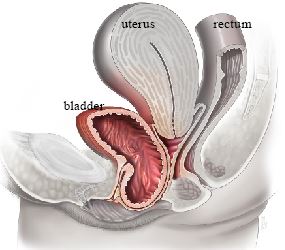
Anterior Compartment Prolapse
Prolapse of the Posterior Compartment
This is when the lower part of the large bowel (rectum) bulges into the back wall of the vagina (which your doctor may refer to as rectocele) and/or part of the small intestine bulges into the upper part of the back wall of the vagina (which your doctor may refer to as enterocele).
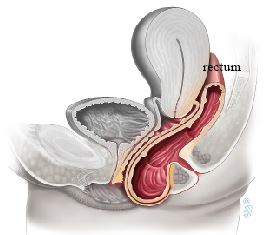
Posterior Compartment Prolapse
Prolapse of the Apical Compartment
- Uterine prolapse. This occurs when the uterus (womb) drops or herniates into the vagina. This is the second most common form of prolapse.
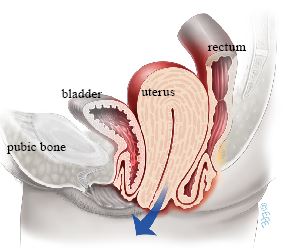
Uterine Prolapse
- Vaginal vault prolapse. Following a hysterectomy, the top of the vagina may collapse downwards, (rather like the toe of a sock turning inside out) falling towards or out of the vaginal opening.
Many women (up to 40%) have a minor degree of prolapse with minimal or no symptoms. Your physician will take a complete medical history and perform a vaginal examination to determine prolapse severity and grade. Different physicians utilize different grading systems and your doctor will explain this to you.
Treatment options can be categorized into non-surgical and surgical options.
Non-surgical Treatment Options
- Do nothing. Prolapse is rarely a life-threatening condition and many women will choose not to have any treatment if they have no symptoms or discomfort. If you have been diagnosed with a prolapse, try to avoid heavy lifting, chronic straining e.g. with constipation, and gaining excess weight as these can cause your prolapse to worsen.
- Pelvic floor exercises (Kegel exercises). Exercising your weakened pelvic floor muscles may help improve or prevent the worsening of early stages of prolapse. Just as with any exercise program, pelvic floor exercises require time, motivation and proper technique. Please see the Pelvic Floor Exercises leaflet for more information.
- Pessary. Pessaries are vaginal devices that come in various shapes and sizes. Pessaries help by providing mechanical support to the prolapsed organs, thus relieving symptoms. Pessaries are most suitable if you wish to delay or avoid surgery, e.g. if your family is not yet complete or if you have medical problems that will make surgery a risk. Pessaries require fitting by your health care provider and may require some trial and error before the most suitable size and type is found for you. It is possible to remain sexually active with some types of pessaries inside the vagina. Please see the Vaginal Pessary for Pelvic Organ Prolapse leaflet for more information.
Ring Pessary
Surgical Treatment Options
For women with symptomatic prolapse, a surgical repair may be offered. Your surgeon will recommend the most appropriate surgical treatment for you based on a number of factors including your age, previous surgical history, severity of prolapse, and your general health. There are two main options: reconstructive surgery and vaginal closure surgery.
- Reconstructive Surgical Repair. The purpose of pelvic reconstructive surgery is to restore your pelvic organs to their natural position while retaining sexual function. There are many ways to accomplish the surgery including:
- Vaginal approach
- Abdominal approach (through an abdominal incision)
- Laparoscopic (keyhole)
- Robotic
- Vaginal Closure Surgery (Colpocleisis). In a few instances your doctor may recommend this surgery, for example, if you have a severe prolapse, are not sexually active and have no intention of becoming sexually active in the future, or if you are medically unfit for reconstructive surgery. During this procedure your surgeon will stitch the vaginal walls together thus preventing the prolapse from recurring. The main advantage of this procedure is its short surgical time and quick recovery. Success rates for this type of procedure are 90 – 95%.
There is no single best approach for all patients. The approach for your particular surgery will depend on many factors, including your history, your surgeon’s training and experience with different approaches, and your preference. Your surgeon will discuss the various options with you and will recommend the type of surgery best suited to your condition and needs. Each repair is individualized; even two different women with the same prolapse may have different needs.
- Vaginal approach. This usually involves making an incision in the vagina, separating the prolapsed organ involved from the vaginal wall and using stitches and or mesh to strengthen and repair the vagina. Permanent stitches may also be placed into the top of the vagina or into the cervix and attached to strong ligaments in the pelvis to provide support to the uterus or vaginal vault (these are termed sacrospinous or uterosacral ligament suspensions).
- Abdominal approach. This involves making an incision in the abdomen and using sutures and/or graft materials to support the vagina, vaginal vault or uterus. In a sacrocolpopexy, a prolapsed vaginal vault is supported using mesh attached to the sacrum. Again, there are many different procedures and your doctor will explain these in detail to you.
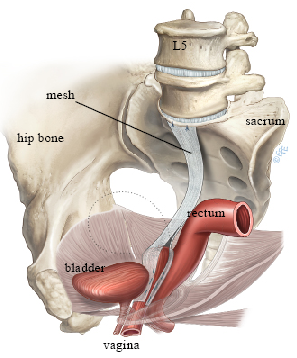
Sacrocolpopexy
- Laparoscopic and robotic approaches. These procedures offer repairs similar to the open abdominal approach but often with quicker recovery time and smaller scars. At present, robotic surgery is only available in a few centers.
It is important to note that the use of vaginal meshes for repair have been withdrawn or restricted in a number of countries including the UK, USA, Australia and New Zealand. Most repairs do not routinely require a graft. Grafts were used in repeat surgeries and where significant risk factors for failure existed with the aim of trying to increase the durability of the repair, but the risk of complications have led to their withdrawal. You should discuss with your surgeon.