
Interstitial Cystitis
In this Health Topic
Interstitial cystitis (IC) is a term used to describe the condition of bladder pain or discomfort with a frequent and urgent need to pass urine. Nine in ten people with IC are women. People with interstitial cystitis may have a bladder wall that is inflamed and irritated (red and painful). In severe cases, the bladder wall inflammation can scar and stiffen the bladder so it can’t easily expand as it fills with urine. Some women get pinpoint bleeding of the bladder wall when it is stretched or have ulcers or fissures of the bladder lining which may lead to pain, urinary frequency and urgency.
Painful Bladder Syndrome (PBS) is another name for the condition when there is no abnormality visible in the bladder. Bladder Pain Syndrome is the name suggested to include both IC and PBS.
People with interstitial cystitis may have many of the following symptoms:
- An urgent need to urinate, both when awake and when asleep, which may be difficult to defer.
- A frequent need to urinate that is out of proportion to liquid consumption.
- Pressure, pain, and tenderness around the bladder, pelvis and perineum (the area between the anus and vagina). These sensations often increase as the bladder fills and decrease as the bladder empties.
- A bladder that won’t hold as much urine as it did before.
- Pain during sexual intercourse.
The symptoms of IC vary greatly from person to person and even in the same individual. In many women, the symptoms get worse before their menstrual period. Stress may also make the symptoms worse, but it doesn’t cause them.
While we don’t currently know the causes of interstitial cystitis, we do know that it is not caused by bacterial or viral infections. Possible causes include a defect in the protective lining of the bladder wall, increased release of histamines, an increased number of nerve cells, and an autoimmune process (when antibodies are made that act against a part of the body) to name a few.
Normally, an inner lining protects the bladder wall from the toxic effects of urine. In about 70% of people with interstitial cystitis, the protective layer lining the bladder is “leaky.” This may let urine irritate the bladder wall, causing interstitial cystitis.
An inflammatory process may increase the release of histamines which result in interstitial cystitis symptoms. There may also be an increased number of nerve cells in the bladder wall which would increase sensitivity.
Your doctor will assess you for the above symptoms, perform testing as needed, and rule out other conditions. Interstitial cystitis is a diagnosis of exclusion.
You may have interstitial cystitis if any of the following occur:
- You have to urinate often or urgently.
- You have persistent pelvic or bladder pain.
- A doctor finds bladder wall inflammation, pinpoint bleeding or ulcers during an exam with a special telescoping camera (called a cystoscope) used to look inside your bladder.
Your doctor has ruled out other diseases such as urinary tract infections, vaginal infections, bladder cancer, and sexually transmitted diseases that may mimic some of the symptoms of interstitial cystitis.
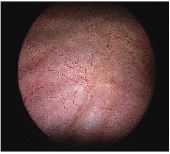
Normal bladder at cystoscopy
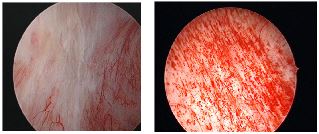
Bladder mucosa (lining) of patients with interstitial cystitis
Because the causes of IC are unknown, current treatments are aimed at relieving symptoms. One or a combination of treatments helps most people for variable periods. As researchers learn more about IC the list of potential treatments will change, so patients should discuss their options with a doctor. Most people feel better after trying one or more of the following treatments:
- Diet. You may need to avoid alcohol, spicy and acidic foods, chocolate, caffeine, citrus drinks, artificial sweeteners, and tomatoes. Try eliminating these foods from your diet for a couple of weeks. Then try eating one food at a time to see if it makes your symptoms worse.
- Quit smoking. Many people with interstitial cystitis find that smoking makes their symptoms worse. Because smoking is also a main cause of bladder cancer, people with interstitial cystitis have another good reason to quit smoking.
- Bladder training. If you have no pain but are bothered by urine frequency or urgency, you may be able to train your bladder to hold more. You can train your bladder by going to the bathroom at scheduled times and using relaxation techniques. After a while, you try to make the time you can wait longer (see Bladder Training leaflet). A physical therapist can help you with bladder training and relaxation techniques as well.
- Physical therapy and biofeedback. People with interstitial cystitis often have painful spasms of the pelvic floor muscles. These can cause pelvic pain and make intercourse uncomfortable. A physical therapist can teach you exercises to both strengthen and relax your pelvic floor muscles.
- Stress Management. Stress reduction, hypnotherapy, and acupuncture can have a beneficial impact for some people.
- Bladder distension. This is a procedure performed under anesthesia, where your bladder is filled very fully with fluid. While about one third of people feel better after having bladder distension, the exact reason why it works is not clear. It may interfere with pain signals sent by nerves in the bladder. Of note, some people feel their pain is worse after this procedure.
- Medication. Your doctor may have you take an oral medicine called pentosan polysulfate. This medicine helps to protect the lining of the bladder wall from the toxic parts of urine. Due to its high cost, it may not be available in some countries. About 40% of patients have an improvement in their symptoms when using pentosan polysulfate. An ophthalmology (eye) exam is recommended before starting pentosan polysulfate due to an associated maculopathy that can develop with use. Another medicine that may help is amitriptiline. It blocks pain and reduces bladder spasms. This medicine can make you sleepy, so it’s usually taken at bedtime. Oral antihistamines or H2 antagonists have also helped some patients with their bladder symptoms. These treatments may work better when the cause of inflammation is allergy based.
- Bladder instillation. During a bladder instillation, a catheter (a thin tube) is used to fill your bladder with a liquid medicine. You hold the medicine inside your bladder for up to 15 minutes, and then the liquid is drained out through the catheter or through urination. Treatments are typically given every one to two weeks for six to eight weeks. The treatment can be repeated as needed. The liquid medicines used can include:
- Heparin alone or in combination.
- Steroids alone or in combination.
- Local anesthetic with or without sodium bicarbonate.
- Liquids containing glycosaminoglycans (the protective layer of the bladder).
- Dimethyl sulfoxide or DMSO, a chemical solvent from wood pulp which has several uses in medicine. It is known to reduce inflammation and block pain in about 3/4 of IC patients. It has the side effect of leaving patients smelling of garlic that may last up to 72 hours after treatment.
- Transcutaneous Electrical Nerve Stimulation (TENS). You can use a TENS machine to put mild electrical pulses over the bladder. Do this at least two times a day. You might do it for a few minutes, or you might do it for a longer time. Ideally, this is commenced under the supervision of a physical therapist.
- Botulinum Toxin. Botulinum toxin injection into the bladder wall is typically performed under anesthesia. The botulinum toxin relaxes the bladder and can decrease urinary frequency bother. This treatment is typically performed 1-2 times per year. Side effects include temporary difficulty emptying the bladder or urinary tract infection.
Some treatments being assessed for people who do not respond to the above options include botulinum toxin bladder injection and sacral nerve stimulation. Some people need stronger pain medication such as morphine-like drugs or gabapentin. Referral to a multidisciplinary pain clinic may be of benefit in severe cases.
An extremely small minority of patients are not helped with regular treatments and require surgery. Many approaches and techniques are used, each of which has its own advantages and complications that should be discussed with your doctor. Surgery should be considered only if all available treatments have failed and the pain is disabling.
The support of family, friends, and other people with interstitial cystitis is very important to help you cope with this problem. People who learn about interstitial cystitis and participate in their own care do better than people who don’t. To find information on IC/BPS support groups in your area, visit the International Painful Bladder Foundation website at www.painful-bladder.org.